
Tech Talk – In Vitro Medical Device Verification Testing in Blood
I previously discussed testing medical devices in blood here (in 2007!), but I think I did a poor job of it and I’d like to revisit it.
Why do you test in blood? Well for one, blood is hard to simulate, it’s a non-Newtonian fluid, and using glycerin and water don’t really do it justice, but these can work depending on the application. For another, a common blood test is to check for hemolysis, sure this is tested during a biocompatibility test, but biocompatibility tests are not performed during actual use conditions. Hemolysis may also be a part of an animal safety study that you want to check out beforehand.
Where do you get the blood from? At a slaughterhouse of course, if you can find a smaller or craft meat location in your area, they’ll probably work with you, one used to sell to us for $40 a week, and we’d take a couple gallon buckets and their workers would fill them up while we waited. They only slaughtered on certain days, so call ahead. You’ll probably find cows easier to find and work with, but there isn’t really a reason you couldn’t use pig blood.
Before we leave for the slaughterhouse we’ll set up a water bath at 37ºC to be ready when we get back. Then we’ll add anticoagulant to the blood collection bucket. We’ll use either heparin or Acid Citrate Dextrose (ACD).
Once we get the blood, we mix the bucket to ensure the anticoagulant is distributed in the blood. Heparin is prescription drug, so hit up your vet consultant or animal lab for some ahead of time. ACD you can make based on USP guidelines from commonly available chemicals (water, citric acid, dextrose, and sodium). We used around 10,000 to 20,000 units of heparin per liter of blood. Of note is heparin is used clinically (on people) more in the U.S. and ACS is used in Europe, so you could maybe argue for the use of one over the other, but you’re using animal blood, so I’m not sure if that really matters. I’ll assume we are using bovine blood for the rest of this post. If you don’t use an anticoagulant, you’ll end up with a clot bucket when you get back to the lab, just throw it away if this happens, it is not recoverable.
Time is generally of the essence so don’t stop by Chili’s on your way back to the lab. Also, just be aware that water will damage your blood cells, so it is preferable to rinse your lab ware with a bit of saline before use.
When we get back to the lab we first check the blood pH and temperature, ideally the pH is between 7.2 and 7.4. We then take a hematocrit (hct) measurement by collecting blood in a capillary tube with clay sealant to stopper the bottom (get blood before using clay). Then we centrifuge the capillary tube for a few minutes at high rpm. Once centrifuged, the capillary tube will look like this:

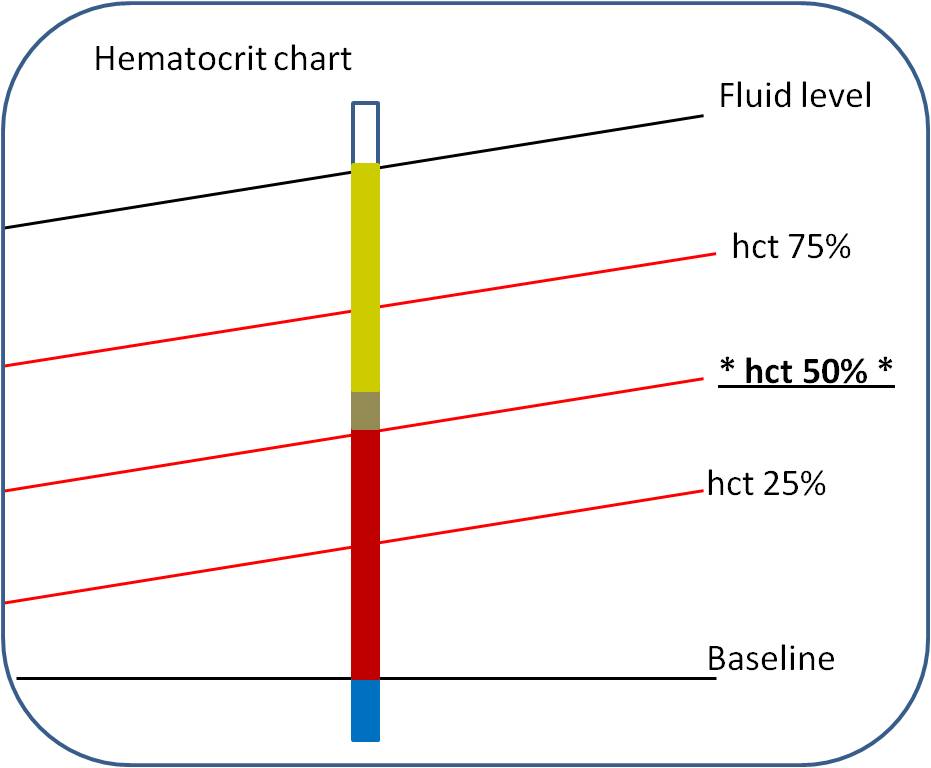
You’ll need a hematocrit chart. Below is a simple representation of how to measure hematocrit, you put the capillary tube on the chart, line up the clay on the baseline, you move the tube left or right until the fluid level matches the top line, then you find the line where the red blood cells stop and follow it over to read the percent hematocrit, in this case 50%.
We generally take two hematocrit measurements and average; you need two capillary tubes to balance the centrifuge anyway. 38 to 42% hct is a typical range for a study like this one, although it will vary depending on how much the animal drank before it was slaughtered, I’ve seen it come in in the low 20s, so don’t worry about the initial hematocrit too much.
We then pump the blood from the collection bucket through a saline primed arterial filter (pediatric filters have lower priming volumes) and line to remove hair and large clots and into a carboy with a plugged outlet at the bottom. We’ll set up a circuit from the bottom of the carboy to the top (through the filter) with a peristaltic pump to keep the blood circulating. Place the outlet in the blood and not above it or you’ll get a bunch of foam. At this point we’ll add saline to the blood to get the hematocrit where we want it, usually around 22% to 32%. Keeping hematocrit consistent is better than not. We’ll measure the hematocrit and adjust until we’re good, using the following formula:
H is the initial hct,
F is the desired hct,
V is the original volume of blood, and
S is the volume of saline to be added.
Once we get the hct where we want, we’ll measure pH and temperature again. At one point we were centrifuging the entire sample to remove the buffy coat layer between the serum and the cells, then mixing it back together but this proved pointless and didn’t really benefit our results or affect our testing any and it was a major pain, so I don’t recommend it.
Once prepared, we can expect the blood to last for five or so hours before it gets questionable. If we’re testing an endovascular device, we’ll pump the blood around a tubing circuit (using a peristaltic pump) and then place the device in the tubing. Preferably the tubing is a similar inner diameter to the artery or vein the device will be used in. You probably want to place the blood reservoir above the test set up and the pump after the test area. Putting the blood reservoir above the test set up ensures a more consistent blood flow. A simple set up is shown below.

We can measure the device performance in blood directly, or we may be interested in something like how much does the device damage the blood, we’ll check the serum and see how red it is in simple terms. If it gets worse over time, then we’re damaging the blood. In this case, for an accurate comparison we need to run a control at the same time. For example, if we have an elaborate pumping system, we’ll run our pump system on one closed circuit and the control (with no device) in another closed circuit and track the hemolysis of both over time.
8 comments:
I read your article which you posted last year but now you explained it with more detail and in easy words.
Keep up the Good Work
I agree is always best to test on blood even if it takes a little more work! Great post...a lot more details and easy to understand.
Sir/Madam,
I have been trying to get some idea for a project on Blood preservation and circulation. I am an Engineering student from Sri Lanka, and i have limited knowledge in the biology side.
In the Medical Device i got one of your paper on In-Vitro test, which impressed me a lot. I would like to receive any other papers in the similar field. And also i would like to know the specification of circuits . Eg: Peristaltic Pump Selection, Temperature Sensor Selection and pH sensor Selection and also about the dealers for these sensors.
Also i would like to get your concern whether you can advise me over the problems and matters during this work period.
Please also direct me to the scientists who are working on similar type of work for me to get some assistance and advice.
Anticipating a favorable reply as soon as possible.
Ur email id is not working. Could u please give me ur contact detail.
Did read the previous post but now clearly understood what point you were trying to make before. If and when a blood glucose level is to be determined can it be diagnosed with the above tests ?
Really great writeup, thanks for sharing.
Good post. I just stumbled upon your blog and wanted to say that I have really enjoyed reading your blog posts. Any way I'll be subscribing to your feed and I hope you post again soon.
Great post. In agreement with Cesar. While the testing in blood may take more work, it is definitely worth the while to do so. Will be subscribing.
Post a Comment